Clinical Focus ›› 2026, Vol. 41 ›› Issue (2): 140-147.doi: 10.3969/j.issn.1004-583X.2026.02.007
Previous Articles Next Articles
The role of dynamic lymphocyte subset monitoring in the full-course management of antineutrophil cytoplasmic antibody-associated vasculitis
Zhang Kaidia, Zhang Lijunb, Chen Lua, Xing Guangquna( )
)
- a. Department of Nephrology, the Affiliated Hospital of Qingdao University, Qingdao 266555, China
b. Department of Critical Care Medicine, the Affiliated Hospital of Qingdao University, Qingdao 266555, China
-
Received:2025-12-18Online:2026-02-20Published:2026-03-05 -
Contact:Xing Guangqun, Email: xinggq@qdu.edu.cn
CLC Number:
Cite this article
Zhang Kaidi, Zhang Lijun, Chen Lu, Xing Guangqun. The role of dynamic lymphocyte subset monitoring in the full-course management of antineutrophil cytoplasmic antibody-associated vasculitis[J]. Clinical Focus, 2026, 41(2): 140-147.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.lchc.cn/EN/10.3969/j.issn.1004-583X.2026.02.007
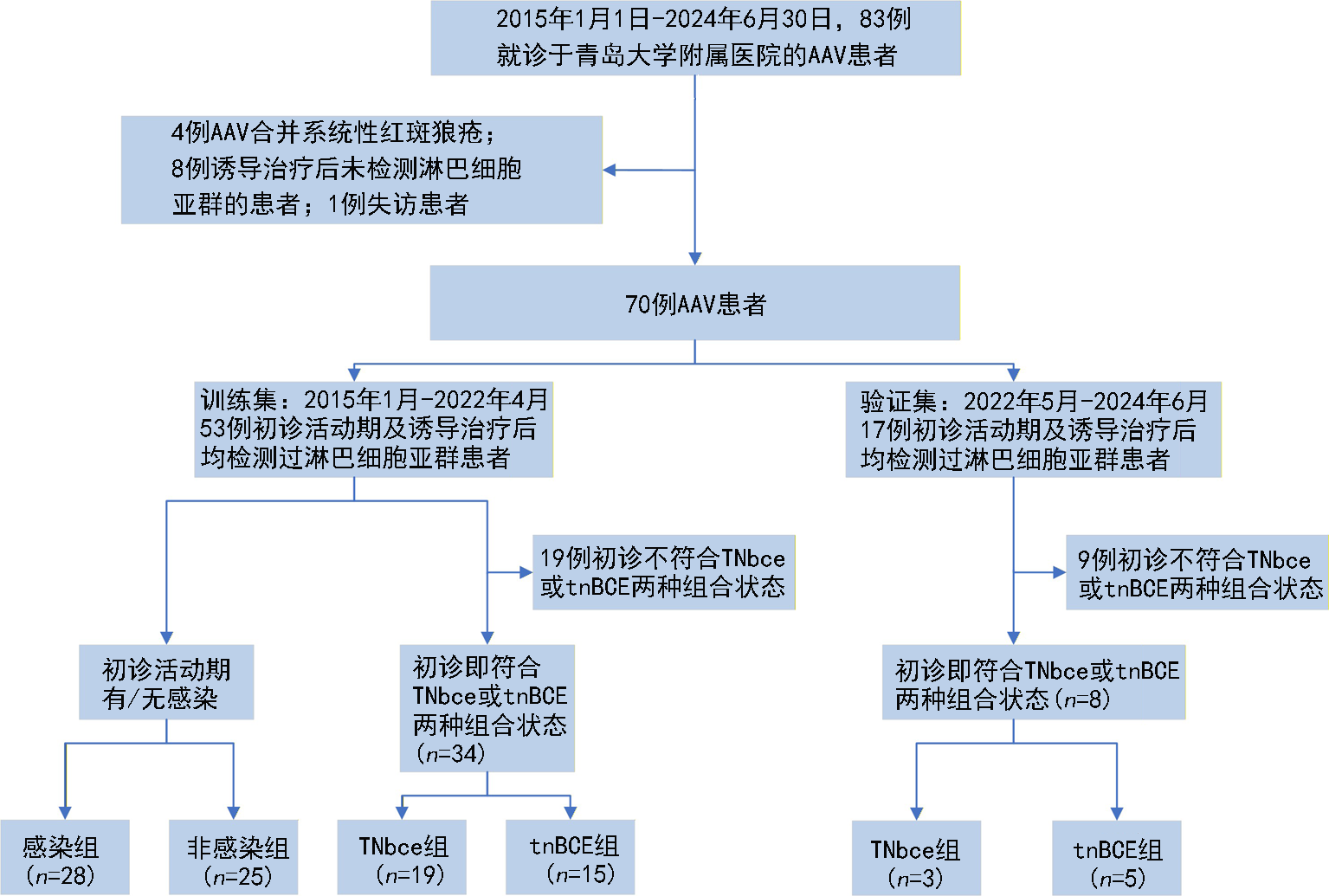
Fig.1 Study flow chart
| 项目 | 初诊时 | 诱导治疗后 | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| BVAS评分(分) | 18.49±4.23 | 9.54±3.81 | -5.063 | <0.001 |
| eGFR[ml/(min·1.73 m2)] | 39.74(22.61,71.98) | 69.22(35.24,119.70) | -4.690 | <0.001 |
| 血肌酐(μmol/L) | 376.70(104.35,579.25) | 212.00(106.82,276.12) | -2.272 | 0.023 |
| CD4+T淋巴细胞计数(cell/μl) | 244.00(190.50,386.00) | 474.50(358.50,838.00) | -2.424 | 0.015 |
| NK细胞(%) | 3.67(1.48,7.64) | 5.66(4.71,18.36) | -2.871 | 0.006 |
| CD8+T淋巴细胞(%) | 28.90(19.15,41.51) | 21.23(19.58,28.07) | -2.389 | 0.017 |
| CD4+T淋巴细胞(%) | 41.66(23.71,54.89) | 47.89(32, 14,72.11) | -4.622 | <0.001 |
| B淋巴细胞(%) | 20.87(1.54,29.29) | 9.17(4.22,20.57) | -3.615 | <0.001 |
| 静止T细胞(%) | 54.20(47.03,62.09) | 57.96(48.08,68.65) | -1.415 | 0.157 |
| 活化T细胞(%) | 13.40(10.07,20.99) | 12.14(9.14,22.82) | -0.223 | 0.823 |
| 活化T感染细胞(%) | 3.07(1.48,4.45) | 1.74(1.02,2.88) | -1.336 | 0.182 |
| 白蛋白(g/L) | 29.30(28.20,32.22) | 32.80(29.70,35.02) | -3.623 | <0.001 |
| D-二聚体(μg/L) | 440.00(250.00,1960.00) | 420.00(267.50,495.00) | -2.823 | 0.005 |
| ESR(mm/h) | 35.50(21.50,106.00) | 12.00(10.00,64.12) | -2.228 | 0.026 |
| CRP(mg/L) | 14.67(6.51,26.03) | 0.94(0.50,21.23) | -2.965 | 0.003 |
| 降钙素原(μg/L) | 0.13(0.07,0.51) | 0.14(0.09,0.16) | -1.087 | 0.282 |
| 血白细胞计数(×109/L) | 6.73(5.95,8.48) | 11.25(8.55,14.25) | -0.295 | 0.693 |
| 血淋巴细胞计数(×109/L) | 0.50(0.47,1.13) | 1.05(0.65,1.64) | -2.941 | 0.003 |
| 血红蛋白(g/L) | 83.53(64.05,102.08) | 103.05(82.57,122.76,) | 3.095 | 0.002 |
| 血小板计数(×109/L) | 187.00(164.00,278.50) | 199.00(174.25,228.75) | -1.311 | 0.190 |
| 尿红细胞计数(个/μl) | 587.80(5.47,587.80) | 148.00(6.05,266.60) | -3.406 | 0.001 |
| 24 h尿蛋白定量(mg/d) | 1 292.80(347.30,2 040.00) | 274.90(221.50,631.72) | -4.042 | <0.001 |
| 补体C3(g/L) | 0.74(0.62,0.87) | 1.03(0.79,1.26) | -2.887 | 0.004 |
| 补体C4(g/L) | 0.19(0.16,0.23) | 0.29(0.26,0.37) | -3.211 | 0.001 |
| IgA(g/L) | 2.08(0.84,2.46) | 2.11(0.80,2.33) | 1.732 | 0.084 |
| IgM(g/L) | 1.28(0.65,2.23) | 1.15(0.56,1.96) | 1.447 | 0.140 |
| IgG(g/L) | 13.58(3.05,19, 45) | 10.34(3.96,18.49) | 0.821 | 0.430 |
| IgE(g/L) | 36.54(19.84,54.00) | 26.70(15.70,62.75) | 1.703 | 0.098 |
| 感染[例(%)] | 28(52.8) | 16(30.2) | 4.262 | 0.039 |
| MPO-ANCA[例(%)] | 14.566 | <0.002 | ||
| +++ | 21(42.9) | 5(10.2) | ||
| ++ | 6(12.2) | 13(26.5) | ||
| + | 10(20.4) | 14(28.6) | ||
| - | 12(24.5) | 17(34.7) | ||
| PR3-ANCA[例(%)] | - | 0.429 | ||
| 阳性 | 4(100.0) | 2(50.0) | ||
| 阴性 | 0 | 2(50.0) |
Tab.1 Comparison of clinical data in the training set at initial diagnosis and after induction therapy(n=53)
| 项目 | 初诊时 | 诱导治疗后 | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| BVAS评分(分) | 18.49±4.23 | 9.54±3.81 | -5.063 | <0.001 |
| eGFR[ml/(min·1.73 m2)] | 39.74(22.61,71.98) | 69.22(35.24,119.70) | -4.690 | <0.001 |
| 血肌酐(μmol/L) | 376.70(104.35,579.25) | 212.00(106.82,276.12) | -2.272 | 0.023 |
| CD4+T淋巴细胞计数(cell/μl) | 244.00(190.50,386.00) | 474.50(358.50,838.00) | -2.424 | 0.015 |
| NK细胞(%) | 3.67(1.48,7.64) | 5.66(4.71,18.36) | -2.871 | 0.006 |
| CD8+T淋巴细胞(%) | 28.90(19.15,41.51) | 21.23(19.58,28.07) | -2.389 | 0.017 |
| CD4+T淋巴细胞(%) | 41.66(23.71,54.89) | 47.89(32, 14,72.11) | -4.622 | <0.001 |
| B淋巴细胞(%) | 20.87(1.54,29.29) | 9.17(4.22,20.57) | -3.615 | <0.001 |
| 静止T细胞(%) | 54.20(47.03,62.09) | 57.96(48.08,68.65) | -1.415 | 0.157 |
| 活化T细胞(%) | 13.40(10.07,20.99) | 12.14(9.14,22.82) | -0.223 | 0.823 |
| 活化T感染细胞(%) | 3.07(1.48,4.45) | 1.74(1.02,2.88) | -1.336 | 0.182 |
| 白蛋白(g/L) | 29.30(28.20,32.22) | 32.80(29.70,35.02) | -3.623 | <0.001 |
| D-二聚体(μg/L) | 440.00(250.00,1960.00) | 420.00(267.50,495.00) | -2.823 | 0.005 |
| ESR(mm/h) | 35.50(21.50,106.00) | 12.00(10.00,64.12) | -2.228 | 0.026 |
| CRP(mg/L) | 14.67(6.51,26.03) | 0.94(0.50,21.23) | -2.965 | 0.003 |
| 降钙素原(μg/L) | 0.13(0.07,0.51) | 0.14(0.09,0.16) | -1.087 | 0.282 |
| 血白细胞计数(×109/L) | 6.73(5.95,8.48) | 11.25(8.55,14.25) | -0.295 | 0.693 |
| 血淋巴细胞计数(×109/L) | 0.50(0.47,1.13) | 1.05(0.65,1.64) | -2.941 | 0.003 |
| 血红蛋白(g/L) | 83.53(64.05,102.08) | 103.05(82.57,122.76,) | 3.095 | 0.002 |
| 血小板计数(×109/L) | 187.00(164.00,278.50) | 199.00(174.25,228.75) | -1.311 | 0.190 |
| 尿红细胞计数(个/μl) | 587.80(5.47,587.80) | 148.00(6.05,266.60) | -3.406 | 0.001 |
| 24 h尿蛋白定量(mg/d) | 1 292.80(347.30,2 040.00) | 274.90(221.50,631.72) | -4.042 | <0.001 |
| 补体C3(g/L) | 0.74(0.62,0.87) | 1.03(0.79,1.26) | -2.887 | 0.004 |
| 补体C4(g/L) | 0.19(0.16,0.23) | 0.29(0.26,0.37) | -3.211 | 0.001 |
| IgA(g/L) | 2.08(0.84,2.46) | 2.11(0.80,2.33) | 1.732 | 0.084 |
| IgM(g/L) | 1.28(0.65,2.23) | 1.15(0.56,1.96) | 1.447 | 0.140 |
| IgG(g/L) | 13.58(3.05,19, 45) | 10.34(3.96,18.49) | 0.821 | 0.430 |
| IgE(g/L) | 36.54(19.84,54.00) | 26.70(15.70,62.75) | 1.703 | 0.098 |
| 感染[例(%)] | 28(52.8) | 16(30.2) | 4.262 | 0.039 |
| MPO-ANCA[例(%)] | 14.566 | <0.002 | ||
| +++ | 21(42.9) | 5(10.2) | ||
| ++ | 6(12.2) | 13(26.5) | ||
| + | 10(20.4) | 14(28.6) | ||
| - | 12(24.5) | 17(34.7) | ||
| PR3-ANCA[例(%)] | - | 0.429 | ||
| 阳性 | 4(100.0) | 2(50.0) | ||
| 阴性 | 0 | 2(50.0) |
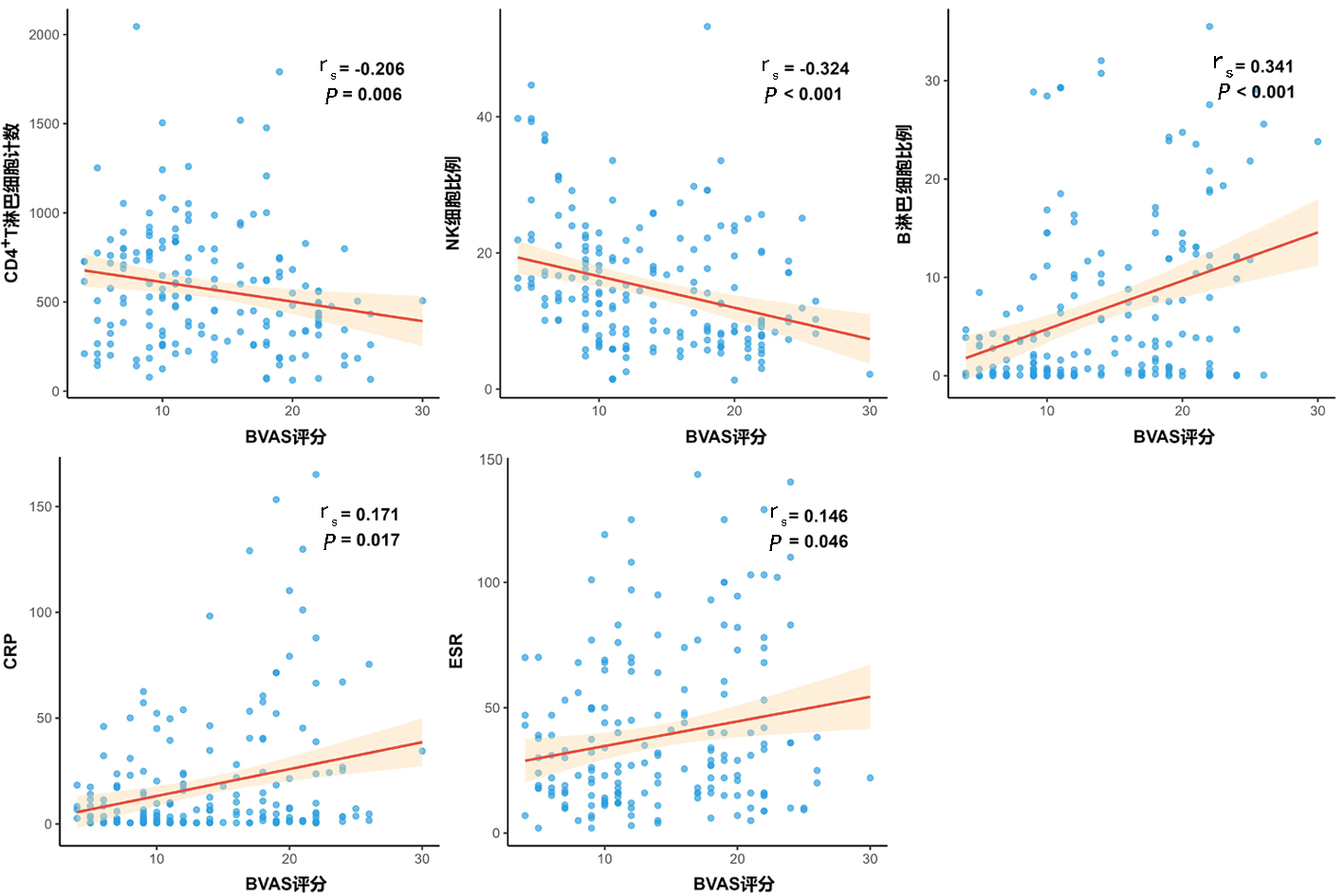
Fig.2 Correlation of lymphocyte subsets and clinical indicators with BVAS scores in newly diagnosed AAV patients
| 项目 | 感染组(n=28) | 非感染组(n=25) | Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 67.00(62.00, 70.5) | 63.00(57.00, 68.00) | -3.708 | <0.001 |
| BVAS评分(分) | 17.61(12.50,23.20) | 14.54(12.21,20.89) | -2.260 | 0.024 |
| eGFR[ml/(min·1.73 m2)] | 46.74(26.61, 71.98) | 57.22(37.24, 119.70) | -2.871 | 0.006 |
| 血肌酐(μmol/L) | 312.00(106.82,476.12) | 244.70(102.36,569.25) | -2.272 | 0.023 |
| CD4+T淋巴细胞计数(cell/μl) | 290.00(160.50,386.00) | 359.00(206.50,508.00) | -2.424 | 0.015 |
| NK细胞(%) | 5.67(1.48,7.64) | 8.87(4.71,18.36) | -2.138 | 0.033 |
| CD8+T淋巴细胞(%) | 27.56(16.15,47.51) | 26.06(18.02,33.53) | -0.855 | 0.392 |
| CD4+T淋巴细胞(%) | 42.73(34.27,51.85) | 46.83(31, 14,71.51) | -2.389 | 0.017 |
| B淋巴细胞(%) | 13.87(5.54,25.43) | 9.86(4.98,16.73) | -2.049 | 0.040 |
| 静止T细胞(%) | 41.61(39.25, 65.15) | 64.43(41.31, 73.33) | -2.450 | 0.014 |
| 活化T细胞(%) | 9.40(5.43,16.04) | 10.14(8.14,22.82) | -0.223 | 0.823 |
| 活化T感染细胞(%) | 8.29(6.32,13.25) | 6.74(3.05,11.88) | -1.336 | 0.182 |
| 白蛋白(g/L) | 30.90(26.41,34.40) | 32.80(28.90,36.10) | -1.356 | 0.176 |
| D-二聚体(μg/L) | 620.00(360.00,2260.00) | 320.00(240.50,560.00) | -2.330 | 0.019 |
| ESR(mm/h) | 46.00(31.30,79.17) | 17.00(11.75,47.00) | -2.242 | 0.024 |
| CRP(mg/L) | 7.67(5.51,32.03) | 1.67(0.51,4.54) | -4.152 | 0.001 |
| 降钙素原(μg/L) | 0.26(0.11,1.04) | 0.09(0.04,0.18) | -2.361 | 0.018 |
| 血白细胞计数(×109/L) | 8.73(5.95,11.61) | 7.14(6.37,9.25) | -2.250 | 0.024 |
| 血淋巴细胞计数(×109/L) | 0.96(0.45,1.24) | 1.30(0.65,1.80) | -3.042 | 0.002 |
| 血红蛋白(g/L) | 87.53(64.05,102.08) | 94.05(82.57,116.76) | -2.171 | 0.030 |
| 血小板计数(×109/L) | 187.00(164.00,278.50) | 199.00(174.25,228.75) | -1.311 | 0.190 |
| 尿红细胞计数(个/μl) | 387.80(5.47,587.80) | 148.00(6.05,266.60) | -3.406 | 0.001 |
| 24 h尿蛋白定量(mg/d) | 892.80(347.30,1 392.00) | 669.90(221.50,1 031.72) | -4.042 | 0.001 |
| 补体C3(g/L) | 0.94(0.62,1.14) | 0.92(0.79,1.18) | -0.581 | 0.561 |
| 补体C4(g/L) | 0.19(0.16,0.23) | 0.23(0.17,0.37) | -0.721 | 0.471 |
| IgA(g/L) | 2.00(0.80,2.56) | 2.09(0.82,2.23) | 1.732 | 0.084 |
| IgM(g/L) | 1.28(0.65,2.23) | 1.25(0.62,1.96) | 0.807 | 0.422 |
| IgG(g/L) | 11.58(3.05,19, 45) | 10.73(3.96,18.49) | -1.350 | 0.176 |
| IgE(g/L) | 32.70(19.84,54.00) | 29.43(17.70,56.75) | 1.703 | 0.098 |
| MPO-ANCA[例(%)] | 5.580 | 0.134 | ||
| +++ | 10(40.0) | 3(12.5) | ||
| ++ | 3(12.0) | 6(25.0) | ||
| + | 6(24.0) | 6(25.0) | ||
| - | 6(24.0) | 9(37.5) | ||
| PR3-ANCA[例(%)] | - | - | ||
| 阳性 | 3(100.0) | 1(100.0) | ||
| 阴性 | 0 | 0 |
Tab.2 Clinical data between the infection group and non-infection group in the training set at initial diagnosis
| 项目 | 感染组(n=28) | 非感染组(n=25) | Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 67.00(62.00, 70.5) | 63.00(57.00, 68.00) | -3.708 | <0.001 |
| BVAS评分(分) | 17.61(12.50,23.20) | 14.54(12.21,20.89) | -2.260 | 0.024 |
| eGFR[ml/(min·1.73 m2)] | 46.74(26.61, 71.98) | 57.22(37.24, 119.70) | -2.871 | 0.006 |
| 血肌酐(μmol/L) | 312.00(106.82,476.12) | 244.70(102.36,569.25) | -2.272 | 0.023 |
| CD4+T淋巴细胞计数(cell/μl) | 290.00(160.50,386.00) | 359.00(206.50,508.00) | -2.424 | 0.015 |
| NK细胞(%) | 5.67(1.48,7.64) | 8.87(4.71,18.36) | -2.138 | 0.033 |
| CD8+T淋巴细胞(%) | 27.56(16.15,47.51) | 26.06(18.02,33.53) | -0.855 | 0.392 |
| CD4+T淋巴细胞(%) | 42.73(34.27,51.85) | 46.83(31, 14,71.51) | -2.389 | 0.017 |
| B淋巴细胞(%) | 13.87(5.54,25.43) | 9.86(4.98,16.73) | -2.049 | 0.040 |
| 静止T细胞(%) | 41.61(39.25, 65.15) | 64.43(41.31, 73.33) | -2.450 | 0.014 |
| 活化T细胞(%) | 9.40(5.43,16.04) | 10.14(8.14,22.82) | -0.223 | 0.823 |
| 活化T感染细胞(%) | 8.29(6.32,13.25) | 6.74(3.05,11.88) | -1.336 | 0.182 |
| 白蛋白(g/L) | 30.90(26.41,34.40) | 32.80(28.90,36.10) | -1.356 | 0.176 |
| D-二聚体(μg/L) | 620.00(360.00,2260.00) | 320.00(240.50,560.00) | -2.330 | 0.019 |
| ESR(mm/h) | 46.00(31.30,79.17) | 17.00(11.75,47.00) | -2.242 | 0.024 |
| CRP(mg/L) | 7.67(5.51,32.03) | 1.67(0.51,4.54) | -4.152 | 0.001 |
| 降钙素原(μg/L) | 0.26(0.11,1.04) | 0.09(0.04,0.18) | -2.361 | 0.018 |
| 血白细胞计数(×109/L) | 8.73(5.95,11.61) | 7.14(6.37,9.25) | -2.250 | 0.024 |
| 血淋巴细胞计数(×109/L) | 0.96(0.45,1.24) | 1.30(0.65,1.80) | -3.042 | 0.002 |
| 血红蛋白(g/L) | 87.53(64.05,102.08) | 94.05(82.57,116.76) | -2.171 | 0.030 |
| 血小板计数(×109/L) | 187.00(164.00,278.50) | 199.00(174.25,228.75) | -1.311 | 0.190 |
| 尿红细胞计数(个/μl) | 387.80(5.47,587.80) | 148.00(6.05,266.60) | -3.406 | 0.001 |
| 24 h尿蛋白定量(mg/d) | 892.80(347.30,1 392.00) | 669.90(221.50,1 031.72) | -4.042 | 0.001 |
| 补体C3(g/L) | 0.94(0.62,1.14) | 0.92(0.79,1.18) | -0.581 | 0.561 |
| 补体C4(g/L) | 0.19(0.16,0.23) | 0.23(0.17,0.37) | -0.721 | 0.471 |
| IgA(g/L) | 2.00(0.80,2.56) | 2.09(0.82,2.23) | 1.732 | 0.084 |
| IgM(g/L) | 1.28(0.65,2.23) | 1.25(0.62,1.96) | 0.807 | 0.422 |
| IgG(g/L) | 11.58(3.05,19, 45) | 10.73(3.96,18.49) | -1.350 | 0.176 |
| IgE(g/L) | 32.70(19.84,54.00) | 29.43(17.70,56.75) | 1.703 | 0.098 |
| MPO-ANCA[例(%)] | 5.580 | 0.134 | ||
| +++ | 10(40.0) | 3(12.5) | ||
| ++ | 3(12.0) | 6(25.0) | ||
| + | 6(24.0) | 6(25.0) | ||
| - | 6(24.0) | 9(37.5) | ||
| PR3-ANCA[例(%)] | - | - | ||
| 阳性 | 3(100.0) | 1(100.0) | ||
| 阴性 | 0 | 0 |
| 变量 | 赋值 |
|---|---|
| 因变量(Y) | |
| 是否发生感染 | 是=1,否=0 |
| 自变量(X) | |
| 年龄 | 连续变量 |
| CD4+T淋巴细胞计数 | 连续变量 |
| NK细胞比例 | 连续变量 |
| B细胞比例 | 连续变量 |
| CRP | 连续变量 |
| ESR | 连续变量 |
Tab.3 Assignment of independent variables and dependent variables in binary multifactor Logistic analysis
| 变量 | 赋值 |
|---|---|
| 因变量(Y) | |
| 是否发生感染 | 是=1,否=0 |
| 自变量(X) | |
| 年龄 | 连续变量 |
| CD4+T淋巴细胞计数 | 连续变量 |
| NK细胞比例 | 连续变量 |
| B细胞比例 | 连续变量 |
| CRP | 连续变量 |
| ESR | 连续变量 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | OR值 | 95%可信区间 | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | 0.088 | 0.032 | 7.282 | 0.007 | 1.092 | 1.024 | 1.163 |
| CD4+T淋巴细胞计数 | -0.001 | 0.001 | 1.487 | 0.223 | 0.999 | 0.998 | 1.001 |
| NK细胞比例 | 0.013 | 0.025 | 0.273 | 0.601 | 1.013 | 0.965 | 1.064 |
| B淋巴细胞比例 | 0.074 | 0.027 | 7.340 | 0.007 | 1.077 | 1.021 | 1.136 |
| CRP | 0.067 | 0.018 | 14.312 | <0.001 | 1.069 | 1.033 | 1.107 |
| ESR | 0.004 | 0.009 | 0.224 | 0.636 | 1.004 | 0.987 | 1.022 |
Tab.4 Multivariate logistic analysis for infection occurrence in AAV patients
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | OR值 | 95%可信区间 | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | 0.088 | 0.032 | 7.282 | 0.007 | 1.092 | 1.024 | 1.163 |
| CD4+T淋巴细胞计数 | -0.001 | 0.001 | 1.487 | 0.223 | 0.999 | 0.998 | 1.001 |
| NK细胞比例 | 0.013 | 0.025 | 0.273 | 0.601 | 1.013 | 0.965 | 1.064 |
| B淋巴细胞比例 | 0.074 | 0.027 | 7.340 | 0.007 | 1.077 | 1.021 | 1.136 |
| CRP | 0.067 | 0.018 | 14.312 | <0.001 | 1.069 | 1.033 | 1.107 |
| ESR | 0.004 | 0.009 | 0.224 | 0.636 | 1.004 | 0.987 | 1.022 |
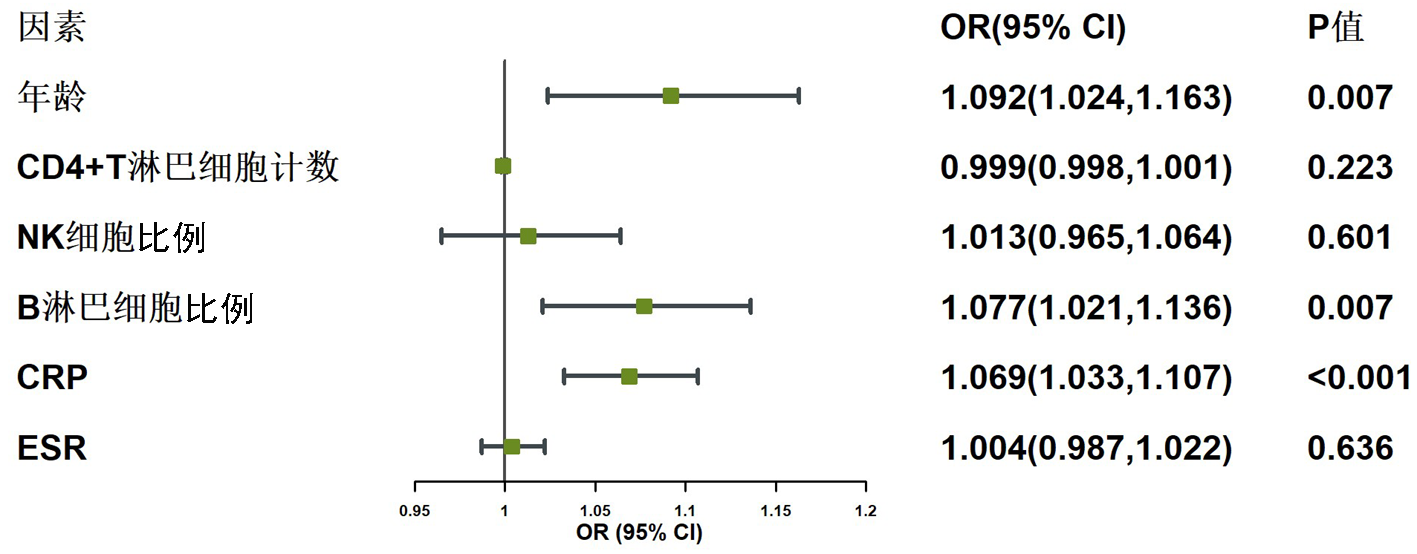
Fig.3 Forest plot of multivariate logistic analysis for infection occurrence in patients with AAV
| 项目 | tnBCE组(n=15) | TNbce组(n=19) | Z/χ2值 | P值 |
|---|---|---|---|---|
| VDI评分(分) | 4.00(3.00, 6.00) | 3.00(2.25, 4.00) | -2.913 | 0.004 |
| BVAS评分(分) | 20.00(12.00, 22.00) | 7.00(5.00, 14.00) | -2.990 | 0.003 |
| 血肌酐(μmol/L) | 264.55(129.55, 346.85) | 119.10(82.00, 175.10) | -2.170 | 0.030 |
| eGFR[ml/(min·1.73 m2)] | 37.69(19.68, 49.20) | 70.96(28.01, 78.91) | -2.590 | 0.010 |
| 白蛋白(g/L) | 29.90(27.05, 33.85) | 36.30(32.80, 39.20) | -4.231 | <0.001 |
| D-二聚体( μg/L) | 1 031.00(577.50, 1 685.00) | 265.00(157.50, 430.00) | -2.387 | 0.017 |
| 血红蛋白(g/L) | 82.00(75.50, 111.00) | 112.00(95.00, 127.00) | -3.014 | 0.003 |
| 降钙素原(μg/L) | 0.60(0.12, 2.17) | 0.06(0.04, 0.67) | -2.927 | 0.003 |
| 尿红细胞计数(个/μl) | 132.70(11.60, 240.60) | 31.90(10.00, 177.47) | -2.228 | 0.022 |
| 24 h尿蛋白定量(g/d) | 1 430.27(1 053.10, 2 440.00) | 116.97(63.20, 271.55) | -3.685 | <0.001 |
| CRP(μg/L) | 12.33(8.56, 25.23) | 0.52(0.50, 0.97) | -5.873 | <0.001 |
| ESR(mm/h) | 40.00(32.60, 68.00) | 6.00(3.00, 11.50) | -4.653 | <0.001 |
| CD4+T淋巴细胞计数(cell/μl) | 176.00(76.80, 300.00) | 673.00(418.40, 768.00) | -5.024 | <0.001 |
| NK细胞(%) | 6.07(2.14, 6.28) | 14.27(9.83, 17.62) | -4.777 | <0.001 |
| B淋巴细胞(%) | 20.05(15.33, 24.26) | 0.02(0.01, 0.05) | -6.514 | <0.001 |
| 血白细胞计数(109/L) | 7.21(5.77, 10.44) | 7.12(6.22, 8.47) | -0.484 | 0.629 |
| 血小板计数(×109/L) | 133.50(114.00, 167.00) | 180.00(111.70, 211.50) | -1.838 | 0.066 |
| 治疗方式[例(%)] | 0.075 | 0.999 | ||
| 激素 | 15(100.0) | 19(100.0) | ||
| RTX | 12(80.0) | 14(73.7) | ||
| CTX | 5(33.3) | 6(31.6) | ||
| 吗替麦考酚酯 | 12(80.0) | 15(79.0) | ||
| 他克莫司 | 2(13.3) | 3(15.8) |
Tab.5 Clinical data between the TNbce group and the tnBCE group
| 项目 | tnBCE组(n=15) | TNbce组(n=19) | Z/χ2值 | P值 |
|---|---|---|---|---|
| VDI评分(分) | 4.00(3.00, 6.00) | 3.00(2.25, 4.00) | -2.913 | 0.004 |
| BVAS评分(分) | 20.00(12.00, 22.00) | 7.00(5.00, 14.00) | -2.990 | 0.003 |
| 血肌酐(μmol/L) | 264.55(129.55, 346.85) | 119.10(82.00, 175.10) | -2.170 | 0.030 |
| eGFR[ml/(min·1.73 m2)] | 37.69(19.68, 49.20) | 70.96(28.01, 78.91) | -2.590 | 0.010 |
| 白蛋白(g/L) | 29.90(27.05, 33.85) | 36.30(32.80, 39.20) | -4.231 | <0.001 |
| D-二聚体( μg/L) | 1 031.00(577.50, 1 685.00) | 265.00(157.50, 430.00) | -2.387 | 0.017 |
| 血红蛋白(g/L) | 82.00(75.50, 111.00) | 112.00(95.00, 127.00) | -3.014 | 0.003 |
| 降钙素原(μg/L) | 0.60(0.12, 2.17) | 0.06(0.04, 0.67) | -2.927 | 0.003 |
| 尿红细胞计数(个/μl) | 132.70(11.60, 240.60) | 31.90(10.00, 177.47) | -2.228 | 0.022 |
| 24 h尿蛋白定量(g/d) | 1 430.27(1 053.10, 2 440.00) | 116.97(63.20, 271.55) | -3.685 | <0.001 |
| CRP(μg/L) | 12.33(8.56, 25.23) | 0.52(0.50, 0.97) | -5.873 | <0.001 |
| ESR(mm/h) | 40.00(32.60, 68.00) | 6.00(3.00, 11.50) | -4.653 | <0.001 |
| CD4+T淋巴细胞计数(cell/μl) | 176.00(76.80, 300.00) | 673.00(418.40, 768.00) | -5.024 | <0.001 |
| NK细胞(%) | 6.07(2.14, 6.28) | 14.27(9.83, 17.62) | -4.777 | <0.001 |
| B淋巴细胞(%) | 20.05(15.33, 24.26) | 0.02(0.01, 0.05) | -6.514 | <0.001 |
| 血白细胞计数(109/L) | 7.21(5.77, 10.44) | 7.12(6.22, 8.47) | -0.484 | 0.629 |
| 血小板计数(×109/L) | 133.50(114.00, 167.00) | 180.00(111.70, 211.50) | -1.838 | 0.066 |
| 治疗方式[例(%)] | 0.075 | 0.999 | ||
| 激素 | 15(100.0) | 19(100.0) | ||
| RTX | 12(80.0) | 14(73.7) | ||
| CTX | 5(33.3) | 6(31.6) | ||
| 吗替麦考酚酯 | 12(80.0) | 15(79.0) | ||
| 他克莫司 | 2(13.3) | 3(15.8) |
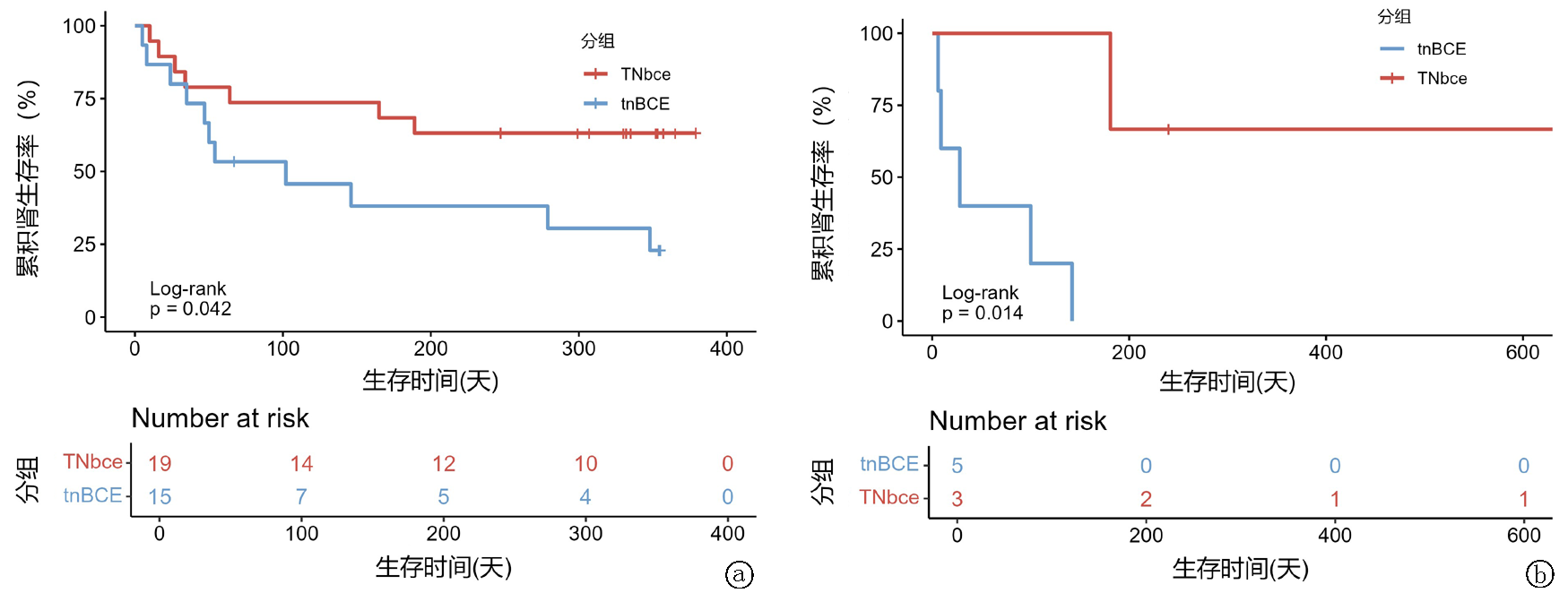
Fig.4 Renal cumulative survival between the tnBCE and TNbce groups a.training set; b.validation set
| [1] | Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus conference nomenclature of vasculitides[J]. Arthritis Rheum, 2013, 65(1): 1-11. doi: 10.1002/art.37715. |
| [2] |
Nakazawa D, Masuda S, Tomaru U, et al. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis[J]. Nat Rev Rheumatol, 2019, 15(2): 91-101. doi: 10.1038/s41584-018-0145-y.
pmid: 30542206 |
| [3] |
Martinez VL, Bordignon DJ, Fulladosa OX, et al. T-lymphocyte in ANCA-associated vasculitis: What do we know? A pathophysiological and therapeutic approach[J]. Clin Kidney J, 2019, 12(4): 503-511. doi: 10.1093/ckj/sfz029.
pmid: 31384441 |
| [4] | Haris Á, Polner K, Arányi J, et al. Incidence and clinical predictors of infections in patients treated with severe systemic ANCA-associated vasculitis[J]. Physiol Int, 2021, 108(1):66-79. doi: 10.1556/2060.2021.00006. |
| [5] |
Caballero-Islas AE, Hoyo-Ulloa I, García-Castro A, et al. Severe infections in patients with anti-neutrophil cytoplasmic antibody-associated vasculitis: A retrospective cohort study with a clinical phenotype approach[J]. Rheumatol Int, 2020, 40(10): 1657-1666. doi: 10.1007/s00296-020-04661-x.
pmid: 32728838 |
| [6] | Xu T, Chen Z, Jiang M, et al. Association between different infection profiles and one-year outcomes in ANCA-associated vasculitis: A retrospective study with monthly infection screening[J]. RMD Open, 2022, 8(2): 1-13. doi: 10.1136/rmdopen-2022-002424. |
| [7] |
Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham vasculitis activity score (version 3)[J]. Ann Rheum Dis, 2009, 68(12):1827-1832. doi:10.1136/ard.2008.101279.
pmid: 19054820 |
| [8] | Exley AR, Bacon PA, Luqmani RA, et al. Development and initial validation of the vasculitis damage index for the standardized clinical assessment of damage in the systemic vasculitides[J]. Arthritis Rheum, 1997, 40(2):371-380. doi: 10.1002/art.1780400222. |
| [9] | 张丽君, 公智卿, 韩润鸿, 等. 淋巴细胞亚群及血细胞比值动态监测对狼疮性肾炎病情判断的价值[J]. 中华全科医师杂志, 2023, 22(12): 1288-1294. doi:10.3760/cma.j.cn114798-20231014-00242. |
| [10] | Patel NJ, Stone JH. Expert perspective: Management of antineutrophil cytoplasmic antibody-associated vasculitis[J]. Arthritis Rheumatol, 2022, 74(8): 1305-1317. doi: 10.1002/art.42114. |
| [11] | Kidney Disease: Improving Global Outcomes (KDIGO) ANCA Vasculitis Work Group. KDIGO 2024 clinical practice guideline for the management of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis[J]. Kidney Int, 2024, 105(3S):S71-S116.doi: 10.1016/j.kint.2023.10.008. |
| [12] | 中华医学会肾脏病学分会专家组. 抗中性粒细胞胞质抗体相关肾炎诊断和治疗中国指南[J]. 中华肾脏病杂志, 2021, (7): 603-620. doi: 10.3760/cma.j.cn441217-20210107-00092. |
| [13] |
London J, Dumoitier N, Lofek S, et al. Skewed peripheral B- and T-cell compartments in patients with ANCA-associated vasculitis[J]. Rheumatology (Oxford), 2021, 60(5): 2157-2168. doi: 10.1093/rheumatology/keaa432.
pmid: 33026090 |
| [14] | Abdulahad WH, Kallenberg CG, Limburg PC, et al. Urinary CD4+ effector memory T cells reflect renal disease activity in antineutrophil cytoplasmic antibody-associated vasculitis[J]. Arthritis Rheum, 2009, 60(9): 2830-2838. doi: 10.1002/art.24747. |
| [15] | Krebs CF, Reimers D, Zhao Y, et al. Pathogen-induced tissue-resident memory T(H)17 (T(RM)17) cells amplify autoimmune kidney disease[J]. Sci Immunol, 2020, 5(50): 1-15. doi: 10.1126/sciimmunol.aba4163. |
| [16] | Vivier E, Raulet DH, Moretta A, et al. Innate or adaptive immunity? The example of natural killer cells[J]. Science, 2011, 331(6013): 6. doi: 10.1126/science.1198687. |
| [17] | Urlaub D, Zhao S, Blank N, et al. Activation of natural killer cells by rituximab in granulomatosis with polyangiitis[J]. Arthritis Res Ther, 2019, 21(1): 277. doi: 10.1186/s13075-019-2054-0. |
| [18] | Merkt W, Salzer U, Thiel J, et al. Blood CD3-(CD56 or 16)+ natural killer cell distributions are heterogeneous in healthy adults and suppressed by azathioprine in patients with ANCA-associated vasculitides[J]. BMC Immunol, 2021, 22(1): 26. doi: 10.1186/s12865-021-00416-w. |
| [19] |
Mcclure M, Gopaluni S, Jayne D, et al. B cell therapy in ANCA-associated vasculitis: Current and emerging treatment options[J]. Nat Rev Rheumatol, 2018, 14(10): 580-591. doi: 10.1038/s41584-018-0065-x.
pmid: 30108367 |
| [20] | 张丽君, 李远, 田芬, 等. 重度活动性狼疮性肾炎冲击治疗淋巴细胞亚群及血细胞比值变化[J]. 青岛大学学报(医学版), 2023, 59(6): 802-807. doi: 10.11712/jms.2096-5532.2023.59.199. |
| [21] | Luan JJ, Xing GQ. Pathogenesis of antimicrobial peptides LL-37 and CpG-ODN in ANCA associated vasculitis[J]. J Nephrol, 2017, 30(1): 63-71. doi: 10.1007/s40620-016-0336-z. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||