Clinical Focus ›› 2026, Vol. 41 ›› Issue (2): 155-159.doi: 10.3969/j.issn.1004-583X.2026.02.009
Previous Articles Next Articles
Youth stroke presenting with seizure-like onset: A case report and literature review
Liu Yijing1,2, Zuo Chun2, Luo Linzheng2,3, Zhao Mingmin4, Ren Bowen2,5, Li Na2,5( )
)
- 1. Graduate School of North China University of Science and Technology, Tangshan 063210, China
2. Neurological Intensive Care Unit, Hebei General Hospital, Shijiazhuang 050051, China
3. Graduate School of Hebei Medical University, Shijiazhuang 050017, China
4. Sixth Department of Neurology, Cangzhou People's Hospital, Cangzhou 061000, China
5. Hebei Provincial Key Laboratory of Cerebral Networks and Cognitive Disorders, Shijiazhuang 050051, China
-
Received:2025-11-03Online:2026-02-20Published:2026-03-05 -
Contact:Li Na, Email: lina0310nicu@163.com
CLC Number:
Cite this article
Liu Yijing, Zuo Chun, Luo Linzheng, Zhao Mingmin, Ren Bowen, Li Na. Youth stroke presenting with seizure-like onset: A case report and literature review[J]. Clinical Focus, 2026, 41(2): 155-159.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.lchc.cn/EN/10.3969/j.issn.1004-583X.2026.02.009
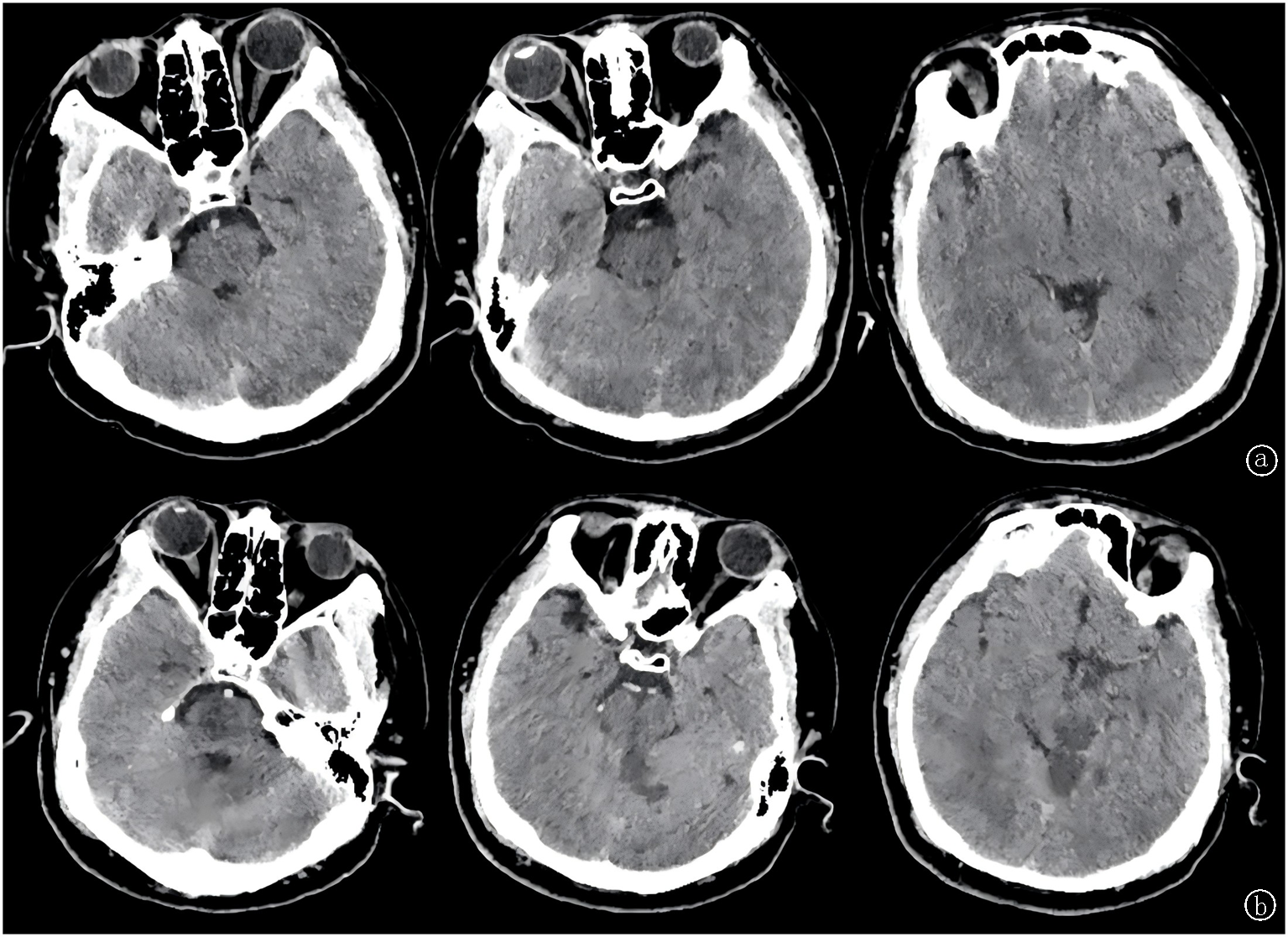
Fig.1 Changes of lesions a. On December 25, 2023, the patient's emergency head CT showed no brain parenchymal lesions; b. On December 26, 2023, the patient's head CT reexamination showed that the low-density shadow of bilateral thalamus, pontine and cerebellum was consistent with the distribution of posterior circulation vessels
| 项目 | 结果 | 参考范围 |
|---|---|---|
| 标准化狼疮抗凝物比值 | 1.19 | 0.8~1.2 |
| 抗β2糖蛋白1抗体IgA/IgM/IgG(AU/ml) | <2.00 | <20 |
| 抗心磷脂抗体IgA(APLU/ml) | <2.50 | <10 |
| 抗心磷脂抗体IgM(MPLU/ml) | <2.00 | <10 |
| 抗心磷脂抗体IgG(GPLU/ml) | <1.00 | <10 |
| 抗环状胍氨酸多肽抗体(U/ml) | <0.5 | ≤5 |
| 抗角蛋白抗体 | 阴性 | 阴性 |
| 抗核抗体 | 阳性1:100 | <1:100=阴性; >1:320=阳性 |
| 抗链球菌溶血素O(U/ml) | 333.00 | 0~200 |
| C反应蛋白(mg/L) | 78.35 | 0~6 |
| 人类免疫缺陷病毒抗体 | 0.03 | <1 |
| 梅毒螺旋抗体 | 0.04 | <1 |
| 毒物分析 | 阴性 | 阴性 |
Tab.1 Etiological screening tests
| 项目 | 结果 | 参考范围 |
|---|---|---|
| 标准化狼疮抗凝物比值 | 1.19 | 0.8~1.2 |
| 抗β2糖蛋白1抗体IgA/IgM/IgG(AU/ml) | <2.00 | <20 |
| 抗心磷脂抗体IgA(APLU/ml) | <2.50 | <10 |
| 抗心磷脂抗体IgM(MPLU/ml) | <2.00 | <10 |
| 抗心磷脂抗体IgG(GPLU/ml) | <1.00 | <10 |
| 抗环状胍氨酸多肽抗体(U/ml) | <0.5 | ≤5 |
| 抗角蛋白抗体 | 阴性 | 阴性 |
| 抗核抗体 | 阳性1:100 | <1:100=阴性; >1:320=阳性 |
| 抗链球菌溶血素O(U/ml) | 333.00 | 0~200 |
| C反应蛋白(mg/L) | 78.35 | 0~6 |
| 人类免疫缺陷病毒抗体 | 0.03 | <1 |
| 梅毒螺旋抗体 | 0.04 | <1 |
| 毒物分析 | 阴性 | 阴性 |
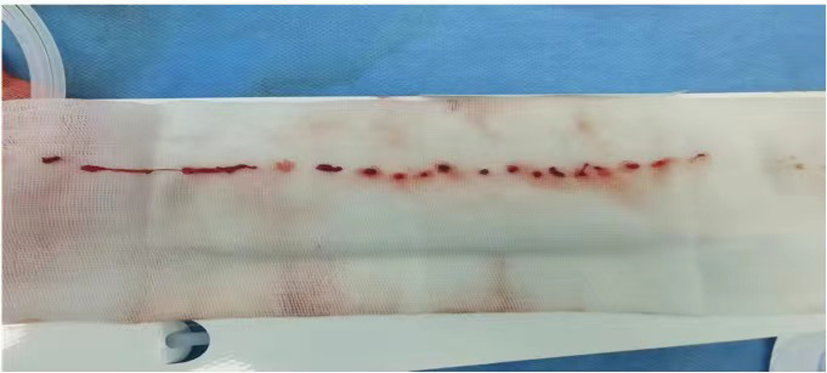
Fig.2 Postoperative thrombosis
| 特征 | 分数(分) |
|---|---|
| 无高血压病史 | 1 |
| 无糖尿病病史 | 1 |
| 无卒中或短暂性脑缺血发作病史 | 1 |
| 非吸烟者 | 1 |
| 影像学上的皮质梗死 | 1 |
| 年龄(岁) | |
| 18~29 | 5 |
| 30~39 | 4 |
| 40~49 | 3 |
| 50~59 | 2 |
| 60~69 | 1 |
| ≥70 | 0 |
Tab.2 RoPE scores
| 特征 | 分数(分) |
|---|---|
| 无高血压病史 | 1 |
| 无糖尿病病史 | 1 |
| 无卒中或短暂性脑缺血发作病史 | 1 |
| 非吸烟者 | 1 |
| 影像学上的皮质梗死 | 1 |
| 年龄(岁) | |
| 18~29 | 5 |
| 30~39 | 4 |
| 40~49 | 3 |
| 50~59 | 2 |
| 60~69 | 1 |
| ≥70 | 0 |
| [1] | Béjot Y, Delpont B, Giroud M. Rising stroke incidence in young adults: More epidemiological evidence, more questions to be answered[J]. J Am Heart Assoc, 2016, 5(5): e003661. doi: 10.1161/JAHA.116.003661. |
| [2] |
Boot E, Ekker MS, Putaala J, et al. Ischaemic stroke in young adults: A global perspective[J]. J Neurol Neurosurg Psychiatry, 2020, 91(4): 411-417.doi: 10.1136/jnnp-2019-322424.
pmid: 32015089 |
| [3] |
Putaala J. Ischemic stroke in young adults[J]. Continuum (Minneap Minn), 2020, 26(2): 386-414.doi: 10.1212/CON.0000000000000833.
pmid: 32224758 |
| [4] | 吴燕平, 彭仕军, 李浩. 特殊的“癫痫”——1例青少年卒中病例报道[J]. 四川医学, 2023, 44(4):445-448.doi:10.16252/j.cnki.issn1004-0501-2023.04.024. |
| [5] | Spengos K, Vemmos K. Risk factors, etiology, and outcome of first-ever ischemic stroke in young adults aged 15 to 45-the athens young stroke registry[J]. Eur J Neurol, 2010, 17( 11): 1358-1364.doi: 10.1111/j.1468-1331.2010.03065.x. |
| [6] |
Ji R, Schwamm LH, Pervez MA, et al. Ischemic stroke and transient ischemic attack in young adults: Risk factors, diagnostic yield, neuroimaging, and thrombolysis[J]. Jama Neurol, 2013, 70( 1): 51-57.doi: 10.1001/jamaneurol.2013.575.
pmid: 23108720 |
| [7] |
Kellert L, Kloss M, Pezzini A, et al. Anemia in young patients with ischaemic stroke[J]. Eur J Neurol, 2015, 22(6):948-953.doi: 10.1111/ene.12687.
pmid: 25712267 |
| [8] |
El-Hattab AW, Adesina AM, Jones J, et al. MELAS syndrome:Clinical manifestations, pathogenesis, and treatment options[J]. Mol Genet Metab, 2015, 116(1-2):4-12.doi: 10.1016/j.ymgme.2015.06.004.
pmid: 26095523 |
| [9] |
Arboix A, Jiménez C, Massons J, et al. Hematological disorders: A commonly unrecognized cause of acute stroke[J]. Expert Rev Hematol, 2016, 9(9):891-901.doi: 10.1080/17474086.2016.1208555.
pmid: 27367035 |
| [10] |
Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults[J]. Lancet Neurol, 2018, 17(9):790-801.doi: 10.1016/S1474-4422(18)30233-3.
pmid: 30129475 |
| [11] | Tsatsakis A, Docea AO, Calina D, et al. A mechanistic and pathophysiological approach for stroke associated with drugs of abuse[J]. J Clin Med, 2019, 8(9):1295-1330.doi: 10.3390/jcm8091295. |
| [12] |
Wolff V, Armspach JP, Beaujeux R, et al. High frequency of intracranial arterial stenosis and cannabis use in ischaemic stroke in the young[J]. Cerebrovasc Dis, 2014, 37(6):438-43.doi: 10.1159/000363618.
pmid: 25059999 |
| [13] | Dutta T, Ryan KA, Thompson O, et al. Marijuana use and the risk of early ischemic stroke:The stroke prevention in young adults study[J]. Stroke, 2021, 52(10):3184-3190.doi: 10.1161/STROKEAHA.120.032811. |
| [14] |
Correia P, Machado S, Meyer I, et al. Ischemic stroke on hormonal contraceptives:Characteristics, mechanisms and outcome[J]. Eur Stroke J, 2021, 6(2):205-212.doi: 10.1177/23969873211019586.
pmid: 34414296 |
| [15] |
Gompel A, Plu-Bureau G. Are we overestimating the stroke risk related to contraceptive pills?[J]. Curr Opin Neurol, 2014, 27(1):29-34.doi: 10.1097/WCO.0000000000000046.
pmid: 24300795 |
| [16] |
Kent DM, Ruthazer R, Weimar C, et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke[J]. Neurology, 2013, 81(7): 619-625.doi: 10.1212/WNL.0b013e3182a08d59.
pmid: 23864310 |
| [17] | Baguley IJ, Perkes IE, Fernandez-Ortega JF, et al. Paroxysmal sympathetic hyperactivity after acquired brain injury: Consensus on conceptual definition, nomenclature, and diagnostic criteria[J]. J Neurotrauma, 2014, 31(17):1515-1520.doi: 10.1089/neu.2013.3301. |
| [18] |
Brás MF, Castro FR, Rita M. Paroxysmal sympathetic hyperactivity: An old but unrecognized condition[J]. Eur J Case Rep Intern Med, 2017, 4(3):562.doi: 10.12890/2017_000562.
pmid: 30755932 |
| [19] |
Baguley IJ. The excitatory:Inhibitory ratio model (EIR model): An integrative explanation of acute autonomic overactivity syndromes[J]. Med Hypotheses, 2008, 70(1): 26-35.doi: 10.1016/j.mehy.2007.04.037.
pmid: 17583440 |
| [20] |
Perkes I, Baguley IJ, Nott MT, et al. A review of paroxysmal sympathetic hyperactivity after acquired brain injury[J]. Ann Neurol, 2010, 68(2): 126-135.doi: 10.1002/ana.22066.
pmid: 20695005 |
| [21] | Baguley IJ, Nicholls JL, Felmingham KL, et al. Dysautonomia after traumatic brain injury: A forgotten syndrome?[J]. J Neurol Neurosurg Psychiatry, 1999, 67(1): 39-43.doi: 10.1136/jnnp.67.1.39. |
| [22] |
Fearnside MR, Cook RJ, McDougall P, et al. The Westmead Head Injury Project outcome in severe head injury. A comparative analysis of pre-hospital, clinical and CT variables[J]. Br J Neurosurg, 1993, 7(3): 267-279.doi: 10.3109/02688699309023809.
pmid: 8338647 |
| [23] |
Baguley IJ, Slewa-Younan S, Heriseanu RE, et al. The incidence of dysautonomia and its relationship with autonomic arousal following traumatic brain injury[J]. Brain Inj, 2007, 21(11): 1175-1181. doi: 10.1080/02699050701687375.
pmid: 17952716 |
| [24] | Tu JSY, Reeve J, Deane AM, et al. Pharmacological management of paroxysmal sympathetic hyperactivity:A scoping review[J]. J Neurotrauma, 2021, 38(16):2221-2237.doi: 10.1089/neu.2020.7597. |
| [25] | Raithel DS, Ohler KH, Porto I, et al. Morphine:An effective abortive therapy for pediatric paroxysmal sympathetic hyperactivity after hypoxic brain injury[J]. J Pediatr Pharmacol Ther, 2015, 20(4):335-340.doi: 10.5863/1551-6776-20.4.335. |
| [26] |
Schroeppel TJ, Sharpe JP, Magnotti LJ, et al. Traumatic brain injury and β-blockers:not all drugs are created equal[J]. J Trauma Acute Care Surg, 2014, 76(2):504-509.doi: 10.1097/TA.0000000000000104.
pmid: 24458058 |
| [27] |
Caldwell SB, Smith D, Wilson FC. Impact of paroxysmal sympathetic hyperactivity on nutrition management after brain injury:A case series[J]. Brain Inj, 2014, 28(3):370-373.doi: 10.3109/02699052.2013.865265.
pmid: 24378107 |
| [28] | Lv LQ, Hou LJ, Yu MK, et al. Hyperbaric oxygen therapy in the management of paroxysmal sympathetic hyperactivity after severe traumatic brain injury:A report of 6 cases[J]. Arch Phys Med Rehabil, 2011, 92(9):1515-1518.doi: 10.1016/j.apmr.2011.01.014. |
| [29] | Wang M, Guo J, Chen SL, et al. Alpha coma after mechanical throm-bectomy for posterior irculation cerebral infarction: A case report and literature review[J]. Asian J Surg, 2022, 45(1): 675-677.doi: 10.1016/j.asjsur.2021.11.019. |
| [30] | 孟坤. 血管内介入治疗后循环急性脑梗死85例临床分析[D]. 长春: 吉林大学, 2014. |
| [31] | Jahan R, Liebeskind DS, Zaidat OO, et al. Stent retriever thrombectomy for anterior vs.posterior circulation ischemic stroke: Analysis of the STRATIS registry[J]. Front Neurol, 2021, 12( 8): 706130-706139.doi: 10.3389/fneur.2021.706130. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||