临床荟萃 ›› 2025, Vol. 40 ›› Issue (9): 837-843.doi: 10.3969/j.issn.1004-583X.2025.09.011
解丽然, 饶小娟, 余玲, 史双伟, 方一凡, 赵明明, 焦培林, 宋淑敏, 桑艳红( )
)
Xie Liran, Rao Xiaojuan, Yu Ling, Shi Shuangwei, Fang Yifan, Zhao Mingming, Jiao Peilin, Song Shumin, Sang Yanhong()
摘要:
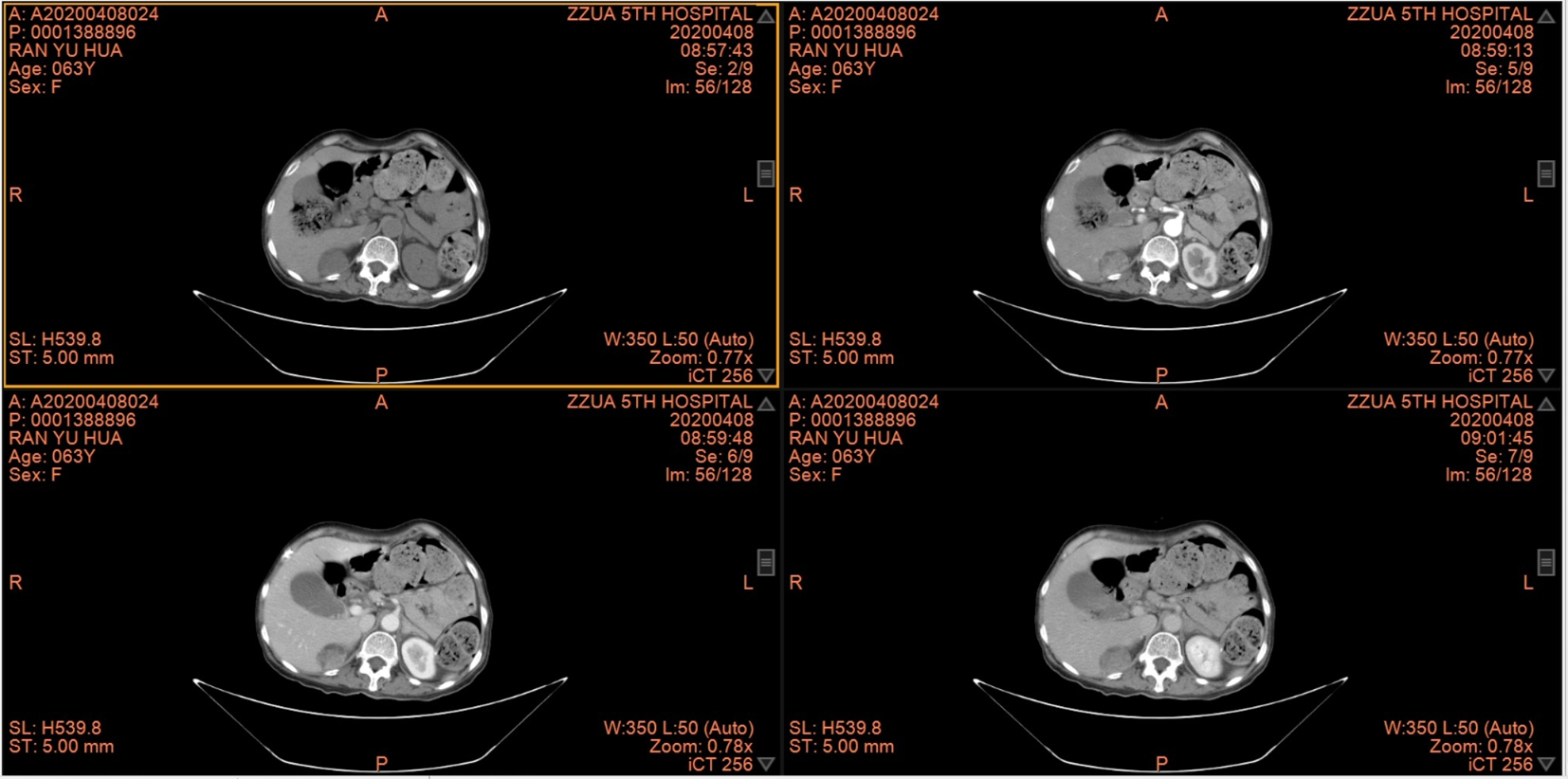
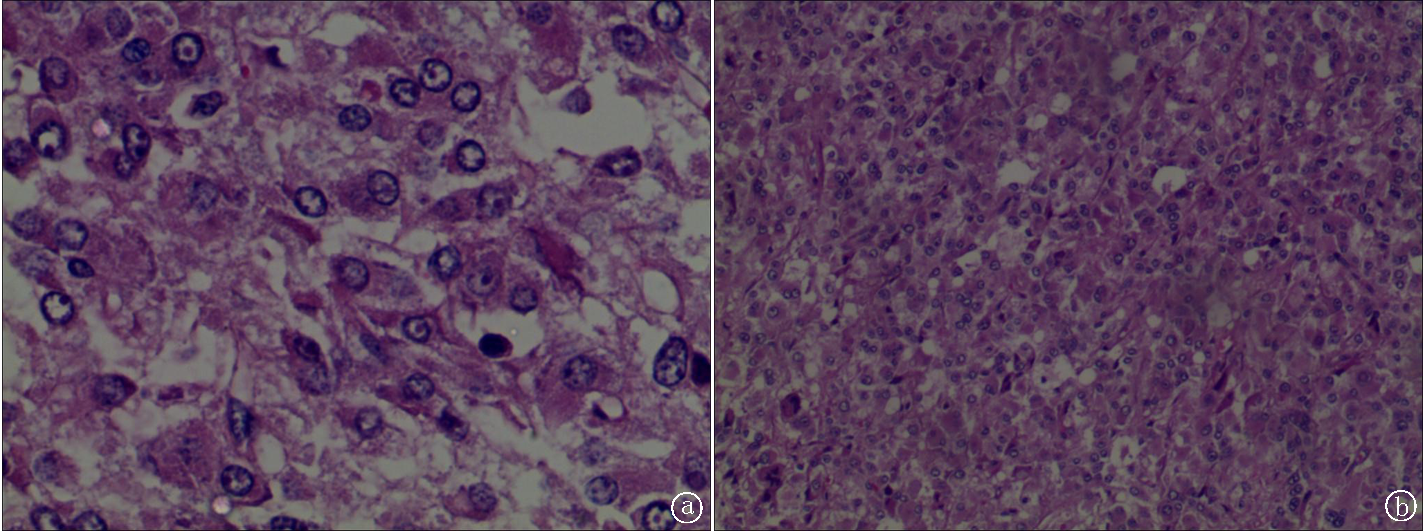
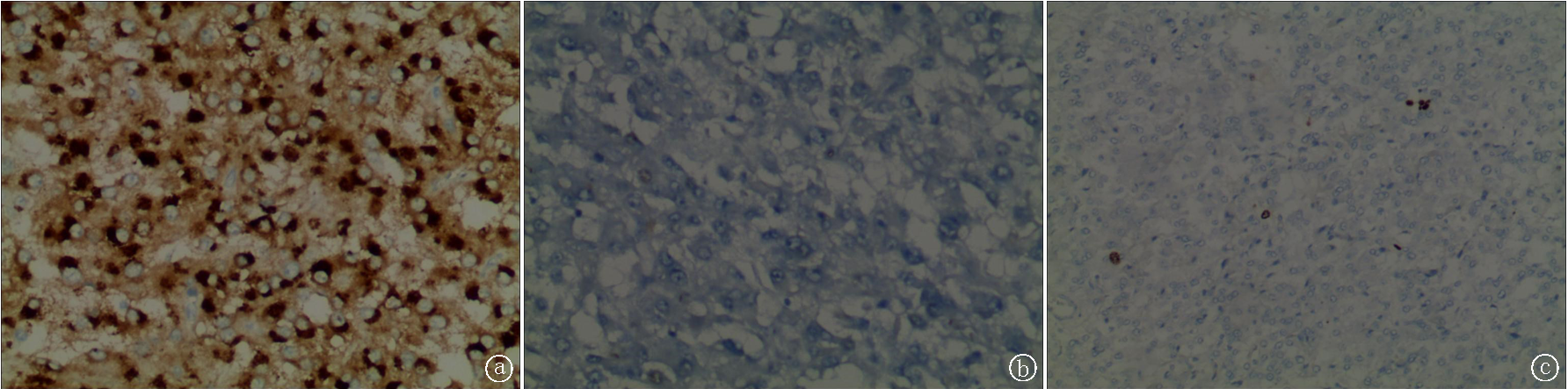
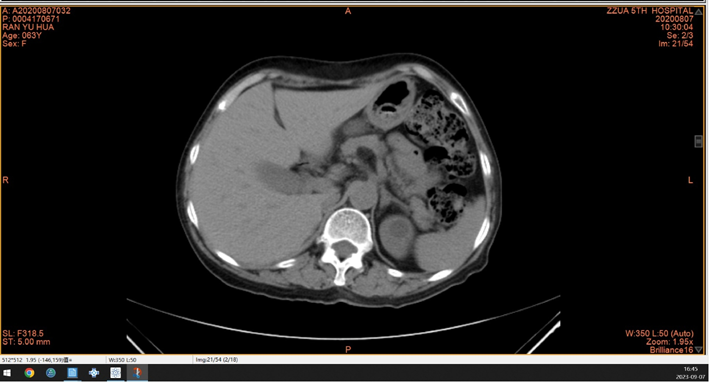
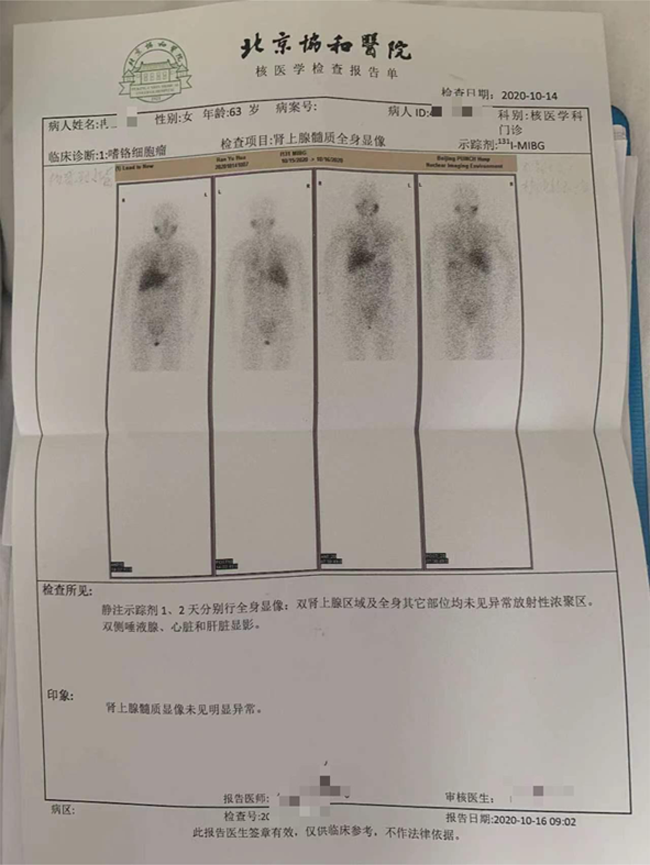
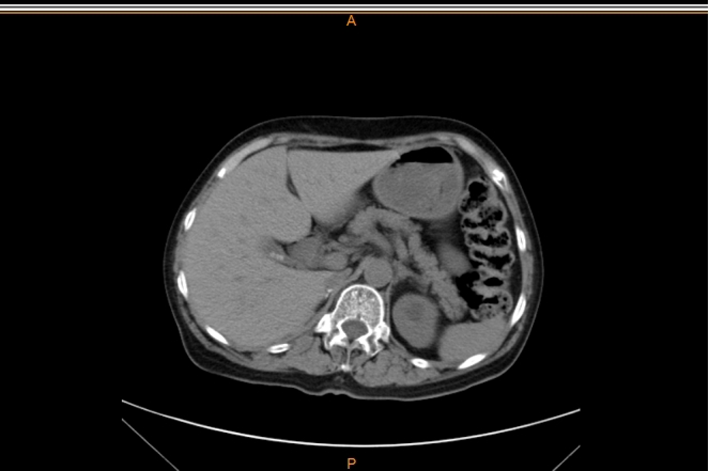
目的 探讨复发性肾上腺嗜铬细胞瘤引起异位促肾上腺皮质激素(adrenocorticotropic hormone, ACTH)综合征的临床诊断和治疗,提高临床医生对该类罕见疾病的认识及重视。方法 回顾性分析1例复发性肾上腺嗜铬细胞瘤致异位ACTH综合征的病例资料,并复习相关文献。结果 患者女性,64岁,因发现血糖高8年,头晕、消瘦2个月入院。既往右侧肾上腺嗜铬细胞瘤术后。患者此次顽固性低钾血症,查ACTH、皮质醇(cortisol, COR)高于检测正常值10倍以上,大、小地塞米松抑制试验不受抑制。血儿茶酚胺六项均明显升高。胸腹联合CT平扫+增强:右侧肾上腺区及右侧肾周多发占位,考虑嗜铬细胞瘤复发及肾周多发转移可能。予常规剂量酚苄明作术前准备,行腹腔镜右侧肾上腺肿瘤切除术。病理提示右侧肾上腺嗜铬细胞瘤,免疫组化CgA(+),NSE(+),Ki-67(+约2%),Sny(+),ACTH(-)。术后ACTH及皮质醇迅速降至正常范围。术后3、6、12个月复查提示儿茶酚胺及ACTH、皮质醇均处于正常范围,患者血压未再升高,血糖较前明显好转,体重逐渐恢复。结论 复发性嗜铬细胞瘤引起异位ACTH综合征是一种罕见疾病,临床遇到异位ACTH综合征需考虑该可能,手术切除是有效治疗手段,术前需按照嗜铬细胞瘤完善术前准备。
中图分类号: