Clinical Focus ›› 2026, Vol. 41 ›› Issue (2): 108-115.doi: 10.3969/j.issn.1004-583X.2026.02.002
Previous Articles Next Articles
Performance of an early quantitative swallowing assessment-based decision tree for predicting stroke-associated pneumonia
Xia Qia, Luo Pingb, Liu Mingfengb, Lin Jiamina, Zhang Weichaoa( )
)
- a. Department of Rehabilitation Medicine, Foshan Sanshui District People's Hospital, Foshan 528100, China
b. Department of Clinical Traditional Chinese Medicine, Foshan Sanshui District People's Hospital, Foshan 528100, China
-
Received:2025-12-11Online:2026-02-20Published:2026-03-05 -
Contact:Zhang Weichao, Email: 505261760@qq.com
CLC Number:
Cite this article
Xia Qi, Luo Ping, Liu Mingfeng, Lin Jiamin, Zhang Weichao. Performance of an early quantitative swallowing assessment-based decision tree for predicting stroke-associated pneumonia[J]. Clinical Focus, 2026, 41(2): 108-115.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.lchc.cn/EN/10.3969/j.issn.1004-583X.2026.02.002
| 项目 | SAP组(n=29) | 非SAP组(n=51) | t/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 65.33±4.51 | 64.82±4.30 | 0.501 | 0.618 |
| 性别[例(%)] | ||||
| 男 | 19(65.5) | 37(72.5) | 0.435 | 0.509 |
| 女 | 10(34.5) | 14(27.5) | ||
| 病程(d) | 42.62±12.87 | 38.77±11.65 | 1.368 | 0.175 |
| BMI(kg/m2) | 23.58±2.12 | 23.10±2.06 | 0.991 | 0.325 |
| 饮酒史[例(%)] | ||||
| 是 | 11(37.9) | 20(39.2) | 0.013 | 0.91 |
| 否 | 18(62.1) | 31(60.8) | ||
| 吸烟史[例(%)] | ||||
| 是 | 9(31.0) | 15(29.4) | 0.023 | 0.879 |
| 否 | 20(69.0) | 36(70.6) | ||
| 糖尿病[例(%)] | ||||
| 是 | 7(24.1) | 13(25.5) | 0.018 | 0.893 |
| 否 | 22(75.9) | 38(74.5) | ||
| 高血脂[例(%)] | ||||
| 是 | 9(31.0) | 18(35.3) | 0.15 | 0.699 |
| 否 | 20(69.0) | 33(64.7) | ||
| 高血压[例(%)] | ||||
| 是 | 24(82.8) | 30(58.8) | 0.216 | 0.642 |
| 否 | 5(17.2) | 11(21.6) | ||
| NIHSS评分(分) | 16.23±2.89 | 15.02±2.74 | 1.862 | 0.066 |
| SSA评分(分) | 28.34±3.25 | 24.65±2.98 | 5.18 | 0 |
| 渗漏[例(%)] | ||||
| 异常 | 14(48.3) | 20(39.2) | 0.621 | 0.431 |
| 正常 | 15(51.7) | 31(60.8) | ||
| 食物残留[例(%)] | ||||
| 异常 | 17(58.6) | 25(49.0) | 0.683 | 0.408 |
| 正常 | 12(41.4) | 26(51.0) | ||
| 吞咽咳嗽反射[例(%)] | ||||
| 异常 | 15(51.7) | 10(19.6) | 8.876 | 0.003 |
| 正常 | 14(48.3) | 41(80.4) | ||
| WST分级[例(%)] | ||||
| Ⅲ~Ⅳ级 | 17(58.6) | 45(88.2) | 9.298 | 0.002 |
| Ⅴ级 | 12(41.4) | 6(11.8) | ||
| 留置胃管[例(%)] | ||||
| 是 | 20(69.0) | 17(33.3) | 9.442 | 0.002 |
| 否 | 9(31.0) | 34(66.7) | ||
| MLR | 0.38±0.10 | 0.34±0.09 | 1.835 | 0.07 |
| NLR | 3.96±1.04 | 2.98±0.90 | 4.423 | 0 |
| PLR | 180.83±35.29 | 169.54±33.87 | 1.412 | 0.162 |
Tab.1 Univariate analysis of clinical data of two groups
| 项目 | SAP组(n=29) | 非SAP组(n=51) | t/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 65.33±4.51 | 64.82±4.30 | 0.501 | 0.618 |
| 性别[例(%)] | ||||
| 男 | 19(65.5) | 37(72.5) | 0.435 | 0.509 |
| 女 | 10(34.5) | 14(27.5) | ||
| 病程(d) | 42.62±12.87 | 38.77±11.65 | 1.368 | 0.175 |
| BMI(kg/m2) | 23.58±2.12 | 23.10±2.06 | 0.991 | 0.325 |
| 饮酒史[例(%)] | ||||
| 是 | 11(37.9) | 20(39.2) | 0.013 | 0.91 |
| 否 | 18(62.1) | 31(60.8) | ||
| 吸烟史[例(%)] | ||||
| 是 | 9(31.0) | 15(29.4) | 0.023 | 0.879 |
| 否 | 20(69.0) | 36(70.6) | ||
| 糖尿病[例(%)] | ||||
| 是 | 7(24.1) | 13(25.5) | 0.018 | 0.893 |
| 否 | 22(75.9) | 38(74.5) | ||
| 高血脂[例(%)] | ||||
| 是 | 9(31.0) | 18(35.3) | 0.15 | 0.699 |
| 否 | 20(69.0) | 33(64.7) | ||
| 高血压[例(%)] | ||||
| 是 | 24(82.8) | 30(58.8) | 0.216 | 0.642 |
| 否 | 5(17.2) | 11(21.6) | ||
| NIHSS评分(分) | 16.23±2.89 | 15.02±2.74 | 1.862 | 0.066 |
| SSA评分(分) | 28.34±3.25 | 24.65±2.98 | 5.18 | 0 |
| 渗漏[例(%)] | ||||
| 异常 | 14(48.3) | 20(39.2) | 0.621 | 0.431 |
| 正常 | 15(51.7) | 31(60.8) | ||
| 食物残留[例(%)] | ||||
| 异常 | 17(58.6) | 25(49.0) | 0.683 | 0.408 |
| 正常 | 12(41.4) | 26(51.0) | ||
| 吞咽咳嗽反射[例(%)] | ||||
| 异常 | 15(51.7) | 10(19.6) | 8.876 | 0.003 |
| 正常 | 14(48.3) | 41(80.4) | ||
| WST分级[例(%)] | ||||
| Ⅲ~Ⅳ级 | 17(58.6) | 45(88.2) | 9.298 | 0.002 |
| Ⅴ级 | 12(41.4) | 6(11.8) | ||
| 留置胃管[例(%)] | ||||
| 是 | 20(69.0) | 17(33.3) | 9.442 | 0.002 |
| 否 | 9(31.0) | 34(66.7) | ||
| MLR | 0.38±0.10 | 0.34±0.09 | 1.835 | 0.07 |
| NLR | 3.96±1.04 | 2.98±0.90 | 4.423 | 0 |
| PLR | 180.83±35.29 | 169.54±33.87 | 1.412 | 0.162 |
| 变量 | 赋值方式 |
|---|---|
| SAP的发生情况 | 非SAP组=“0”;SAP组=“1” |
| SSA评分 | 实测值 |
| 吞咽咳嗽反射 | 正常=“0”;异常=“1” |
| WST分级 | Ⅲ-Ⅳ级=“0”;Ⅴ级=“1” |
| 留置胃管 | 否=“0”;是=“1” |
| NLR | 实测值 |
Tab.2 Variable assignment table
| 变量 | 赋值方式 |
|---|---|
| SAP的发生情况 | 非SAP组=“0”;SAP组=“1” |
| SSA评分 | 实测值 |
| 吞咽咳嗽反射 | 正常=“0”;异常=“1” |
| WST分级 | Ⅲ-Ⅳ级=“0”;Ⅴ级=“1” |
| 留置胃管 | 否=“0”;是=“1” |
| NLR | 实测值 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | OR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| SSA评分 | 0.442 | 0.137 | 10.426 | 0.001 | 1.555 | 1.190 | 2.033 |
| 吞咽咳嗽反射 | 2.306 | 0.852 | 7.326 | 0.007 | 10.036 | 1.889 | 53.306 |
| WST分级Ⅴ级 | 2.015 | 0.968 | 4.330 | 0.037 | 7.499 | 1.124 | 50.030 |
| 留置胃管 | 1.760 | 0.842 | 4.375 | 0.036 | 5.814 | 1.117 | 30.263 |
| NLR | 1.109 | 0.402 | 7.597 | 0.006 | 3.031 | 1.378 | 6.669 |
| 常量 | -18.168 | 4.527 | 16.103 | 0.000 | 0.000 | ||
Tab.3 Multivariate logistic regression analysis of SAP in CVA patients with swallowing dysfunction
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | OR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| SSA评分 | 0.442 | 0.137 | 10.426 | 0.001 | 1.555 | 1.190 | 2.033 |
| 吞咽咳嗽反射 | 2.306 | 0.852 | 7.326 | 0.007 | 10.036 | 1.889 | 53.306 |
| WST分级Ⅴ级 | 2.015 | 0.968 | 4.330 | 0.037 | 7.499 | 1.124 | 50.030 |
| 留置胃管 | 1.760 | 0.842 | 4.375 | 0.036 | 5.814 | 1.117 | 30.263 |
| NLR | 1.109 | 0.402 | 7.597 | 0.006 | 3.031 | 1.378 | 6.669 |
| 常量 | -18.168 | 4.527 | 16.103 | 0.000 | 0.000 | ||
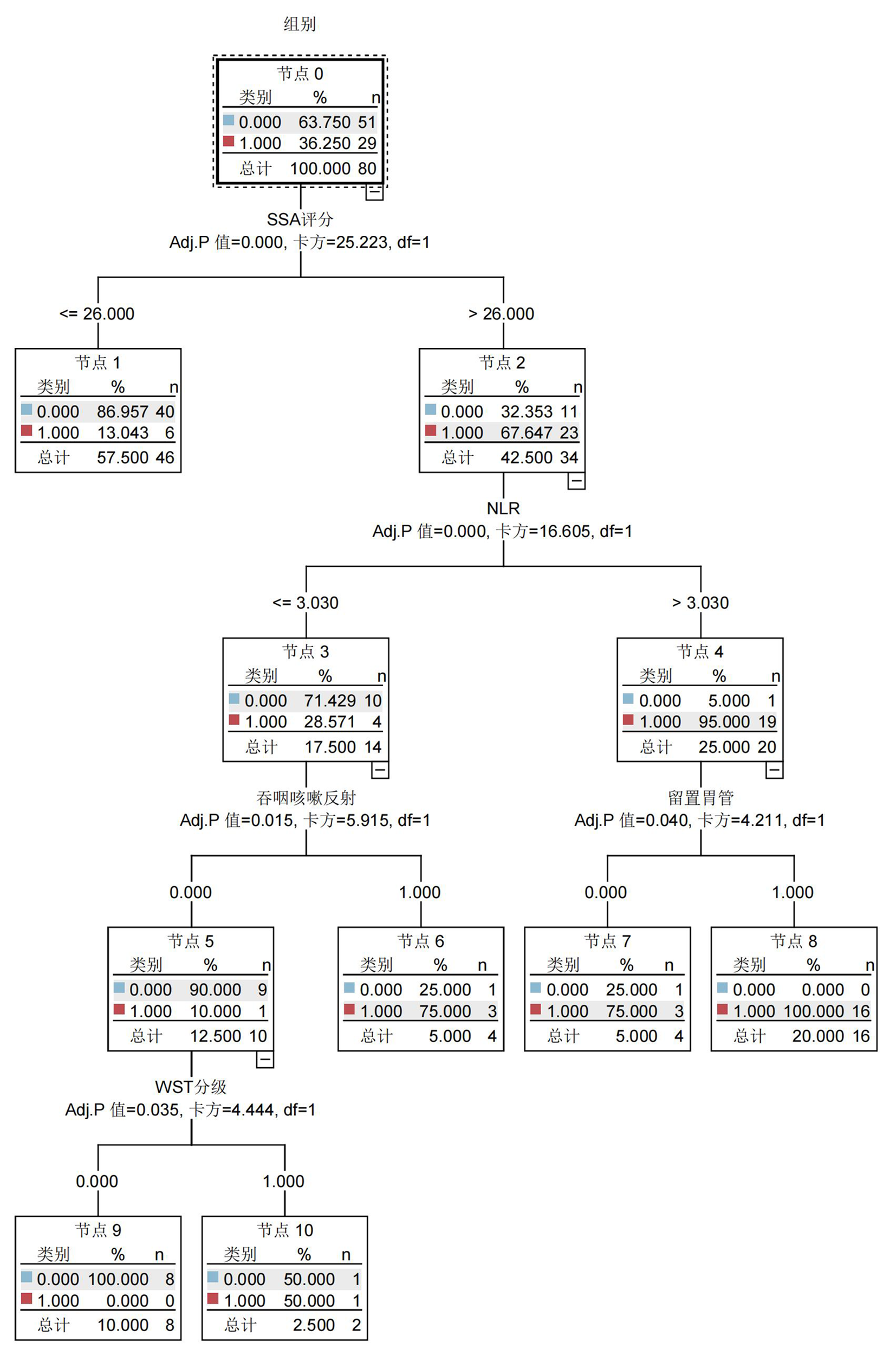
Fig.1 The decision tree model of SAP in CVA patients with swallowing dysfunction
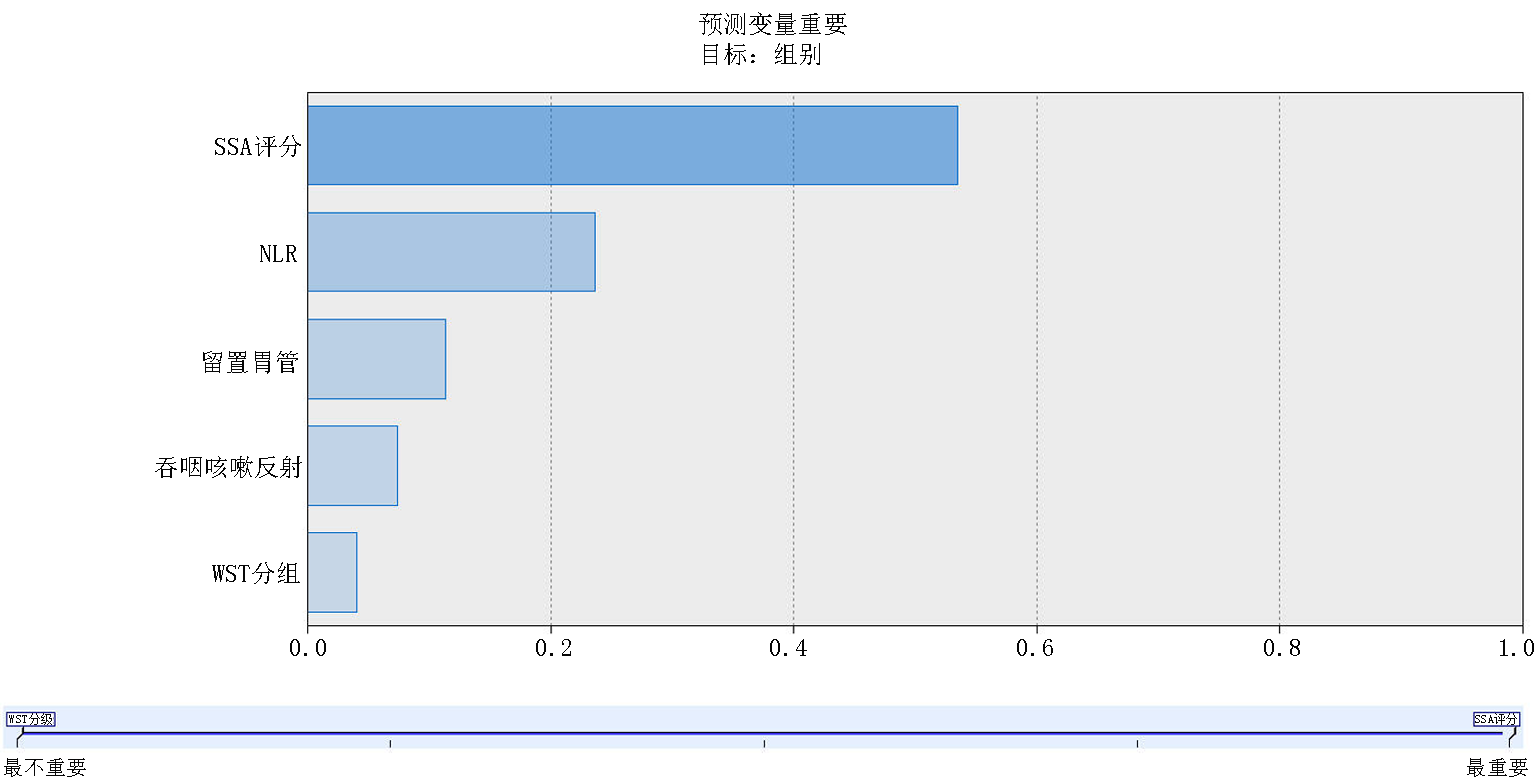
Fig.2 Ranking of the importance of predictor variables
| 模型 | AUC | 标准误 | P值 | 95%CI |
|---|---|---|---|---|
| 决策树模型 | 0.925 | 0.031 | <0.01 | 0.844~0.972 |
| logistic回归模型 | 0.847 | 0.047 | <0.01 | 0.749~0.918 |
Tab.4 Predictive efficacy of decision tree model and logistic regression model
| 模型 | AUC | 标准误 | P值 | 95%CI |
|---|---|---|---|---|
| 决策树模型 | 0.925 | 0.031 | <0.01 | 0.844~0.972 |
| logistic回归模型 | 0.847 | 0.047 | <0.01 | 0.749~0.918 |
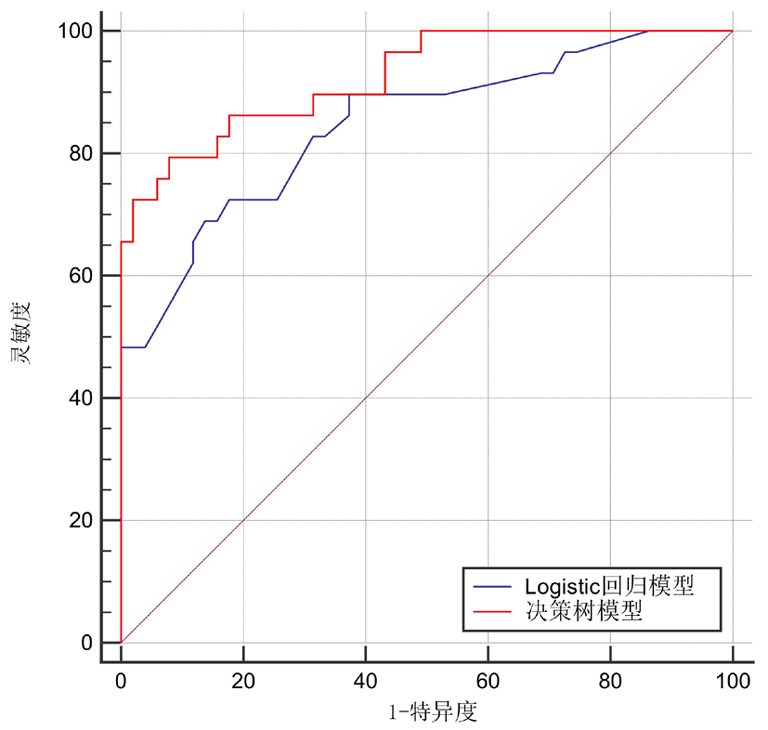
Fig.3 The ROC curves for the decision tree model and the logistic regression model
| [1] | Dogariu OA, Dogariu I, Vasile CM, et al. Diagnosis and treatment of watershed strokes:AA narrative review[J]. J Med Life, 2023, 16(6):842-850.doi: 10.25122/jml-2023-0127. |
| [2] | Anderson CS. Progress-defining risk factors for stroke prevention[J]. Cerebrovasc Dis, 2021, 50(6):615-616. doi: 10.1159/000516996. |
| [3] | D'Netto P, Rumbach A, Dunn K, et al. Clinical predictors of dysphagia recovery after stroke: A systematic review[J]. Dysphagia, 2023, 38(1):1-22.doi: 10.1007/s00455-022-10443-3. |
| [4] | Eltringham SA, Bray BD, Smith CJ, et al. Are differences in dysphagia assessment, oral care provision, or nasogastric tube insertion associated with stroke-associated pneumonia? A nationwide survey linked to national stroke registry data[J]. Cerebrovasc Dis, 2022, 51(3):365-372.doi: 10.1159/000519903. |
| [5] |
Schumann-Werner B, Becker J, Nikoubashman O, et al. The relationship between neurogenic dysphagia, stroke-associated pneumonia and functional outcome in a cohort of ischemic stroke patients treated with mechanical thrombectomy[J]. J Neurol, 2023, 270(12):5958-5965.doi: 10.1007/s00415-023-11940-7.
pmid: 37632565 |
| [6] | Jannini TB, Ruggiero M, Viganò A, et al. The role of the Sapienza GLObal Bedside Evaluation of Swallowing after Stroke (GLOBE-3S) in the prevention of stroke-associated pneumonia (SAP)[J]. Neurol Sci, 2022, 43(2):1167-1176.doi: 10.1007/s10072-021-05449-y. |
| [7] | Wang J, Chang E, Jiang Y. Effects of vitamin C stimulation on rehabilitation of dysphagia after stroke: Arandomized trial[J]. Eur J Phys Rehabil Med, 2022, 58(4):558-564.doi: 10.23736/S1973-9087.22.07337-3. |
| [8] |
Flayer CH, Perner C, Sokol CL. A decision tree model for neuroimmune guidance of allergic immunity[J]. Immunol Cell Biol, 2021, 99(9):936-948.doi: 10.1111/imcb.12486.
pmid: 34115905 |
| [9] | 全国第四届脑血管病学术会议. 各类脑血管疾病诊断要点[J]. 中华神经科杂志, 1996, 29(6):379-381. |
| [10] | 中国卒中学会急救医学分会, 中华医学会急诊医学分会卒中学组, 中国老年医学学会急诊医学分会, 等. 卒中相关性肺炎诊治中国专家共识(2019更新版)[J]. 中国急救医学, 2019, 39(12):1135-1143. |
| [11] | Alemseged F, Rocco A, Arba F, et al. Basilar Artery Treatment and Management (BATMAN) collaboration investigators. Posterior national institutes of health stroke scale improves prognostic accuracy in posterior circulation stroke[J]. Stroke, 2022, 53(4):1247-1255.doi: 10.1161/STROKEAHA.120.034019. |
| [12] | Tai J, Hu R, Fan S, et al. Theta-burst transcranial magnetic stimulation for dysphagia patients during recovery stage of stroke:AA randomized controlled trial[J]. Eur J Phys Rehabil Med, 2023, 59(5):543-553.doi: 10.23736/S1973-9087.23.08023-1. |
| [13] |
Labeit B, Michou E, Trapl-Grundschober M, et al. Dysphagia after stroke: Research advances in treatment interventions[J]. Lancet Neurol, 2024, 23(4):418-428.doi: 10.1016/S1474-4422(24)00053-X.
pmid: 38508837 |
| [14] | 赵林娟, 顾永梅, 葛春霞, 等. 脑卒中吞咽障碍患者相关性肺炎危险因素分析及其预防策略[J]. 中华保健医学杂志, 2023, 25(1):97-99. |
| [15] | 王甜梦, 曾泓辑, 李彩霞, 等. 脑卒中后吞咽障碍患者吸入性肺炎的影响因素分析及预测模型构建[J]. 中华物理医学与康复杂志, 2024, 46(7):618-623. |
| [16] | 孔玉明, 李治璋, 岳蕴华. 急性缺血性脑卒中静脉溶栓患者并发卒中相关性肺炎的危险因素分析[J]. 中风与神经疾病杂志, 2021, 38(8):693-695. doi:10.19845/j.cnki.zfysjjbzz.2021.0184. |
| [17] |
Patel UK, Kodumuri N, Dave M, et al. Stroke-associated pneumonia: A retrospective study of risk factors and outcomes[J]. Neurologist, 2020, 25(3):39-48.doi: 10.1097/NRL.0000000000000269.
pmid: 32358460 |
| [18] |
么美康, 尹丽丽. 老年卒中相关性肺炎患者多重耐药菌感染危险因素研究进展[J]. 临床荟萃, 2023, 38(1):84-87.
doi: 10.3969/j.issn.1004-583X.2023.01.014 |
| [19] | 高新梅, 邢雷, 王清涛, 等. 脑卒中相关性肺炎患者多药耐药菌感染影响因素分析及预测模型构建[J]. 检验医学与临床, 2025, 22(4):475-484. |
| [20] | 于凯娜, 高耐芬, 范素芳, 等. 早期肺康复干预治疗老年2型糖尿病合并卒中相关性肺炎患者的疗效观察[J]. 中华保健医学杂志, 2024, 26(6):765-768. |
| [21] | 段霞, 侯景明, 洪健, 等. 脑卒中后吞咽障碍患者发生相关性肺炎的危险因素及预测模型分析[J]. 中国康复医学杂志, 2022, 37(5):616-622. |
| [22] | 李晨红, 姜晨黎, 王金慧, 等. 脑出血患者微创颅内血肿清除术后肺部感染的影响因素分析及预测模型构建[J]. 中国卒中杂志, 2024, 19(5):532-538. |
| [23] | 任向利, 任向杰, 白玉, 等. 卒中相关性肺炎临床特点及危险因素分析[J]. 解放军医药杂志, 2021, 33(1):44-48. |
| [24] | 涂秀, 张克昌, 吴战. 胃肠疾病手术患者术后呼吸道感染的病原菌分布药敏性及影响因素分析[J]. 河北医学, 2023, 29(12):2077-2083. |
| [25] | 李园, 马婷, 杨媛. 慢性支气管炎患者合并肺部感染后肺功能与免疫反应的变化及对预后的影响[J]. 中国医刊, 2025, 60(2):144-148. |
| [26] | 陈左然, 张晔, 王铁军, 等. 探讨NPAR、NLR对老年缺血性脑卒中相关性肺炎患者的预测价值[J]. 脑与神经疾病杂志, 2023, 31(11):703-708. |
| [27] | Wang K, Liu Q, Mo S, et al. A decision tree model to help treatment decision-making for severe spontaneous intracerebral hemorrhage[J]. Int J Surg, 2024, 110(2):788-798.doi: 10.1097/JS9.0000000000000852. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||